Relieve Pressure, Restore Function, and Feel Supported
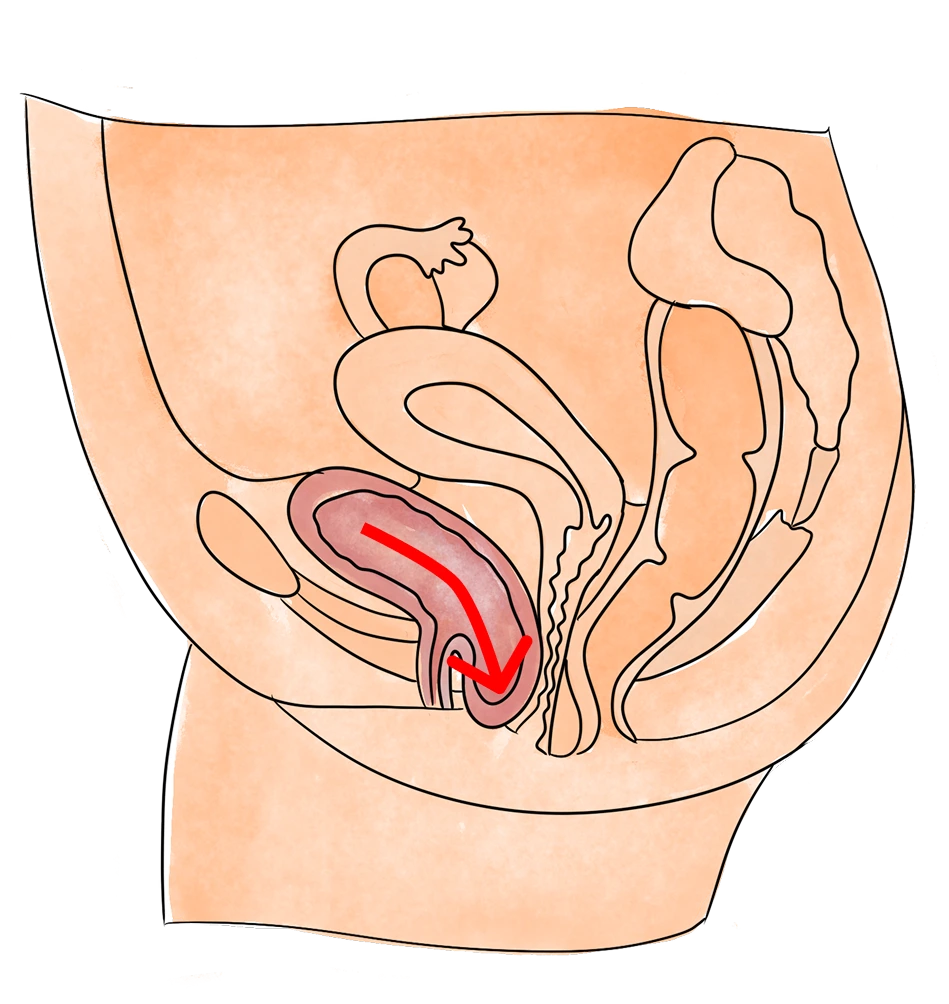
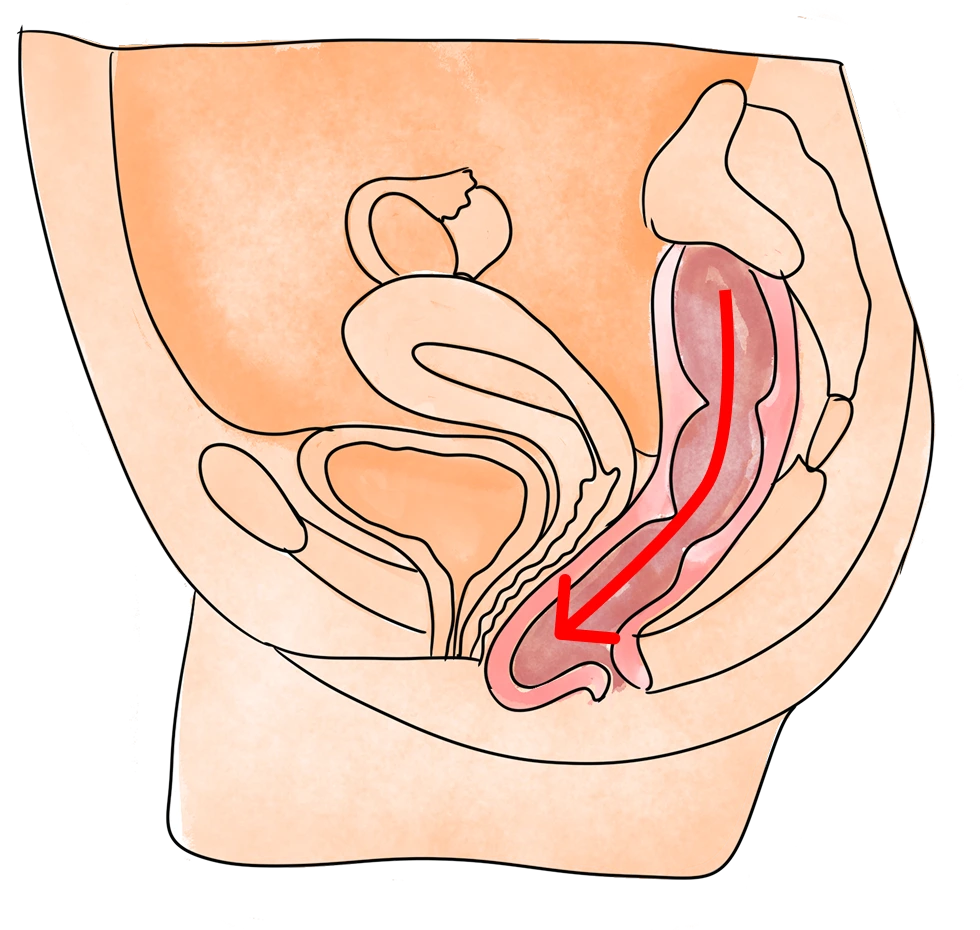
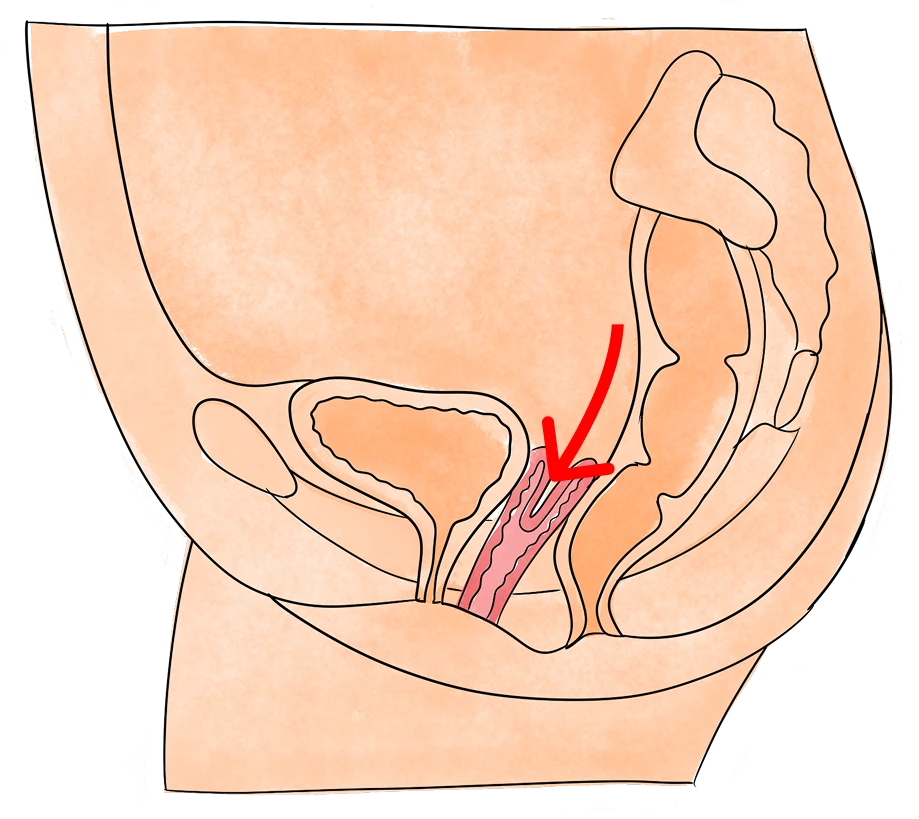
Pelvic organ prolapse (POP) occurs when one or more of the pelvic organs—such as the bladder, uterus, or rectum—descends and presses against the vaginal or rectal wall due to weakness or dysfunction of the pelvic floor muscles and connective tissue.
Prolapse is often associated with childbirth, menopause, heavy lifting, chronic constipation, or prior pelvic surgeries. While common, prolapse is not inevitable—and many cases can be effectively managed without surgery.
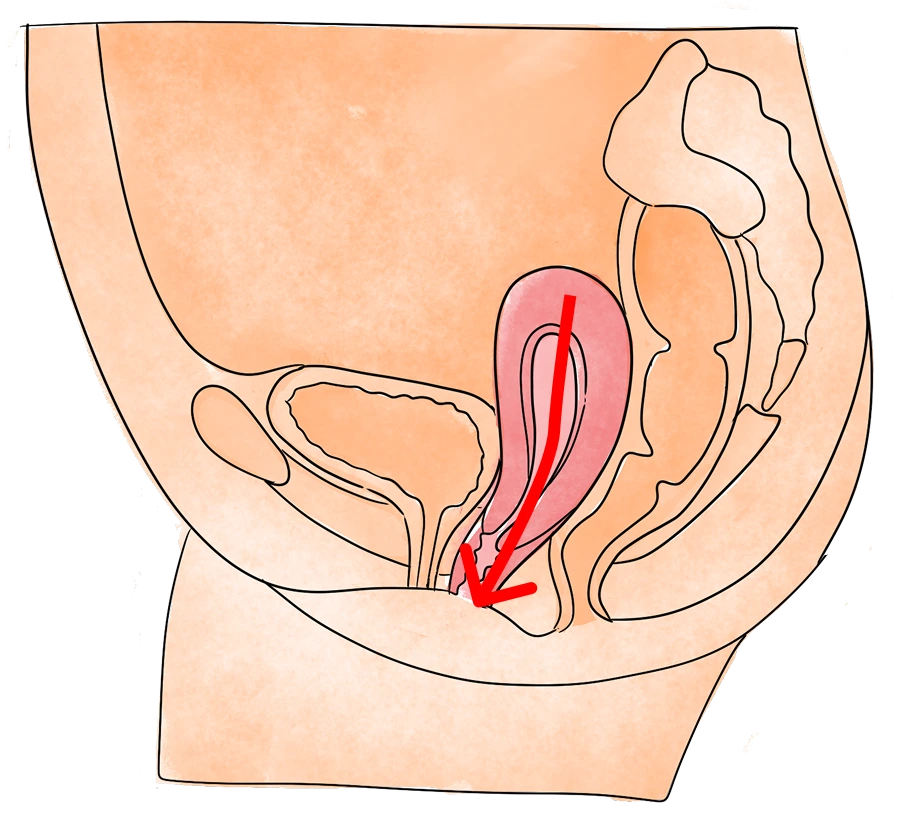
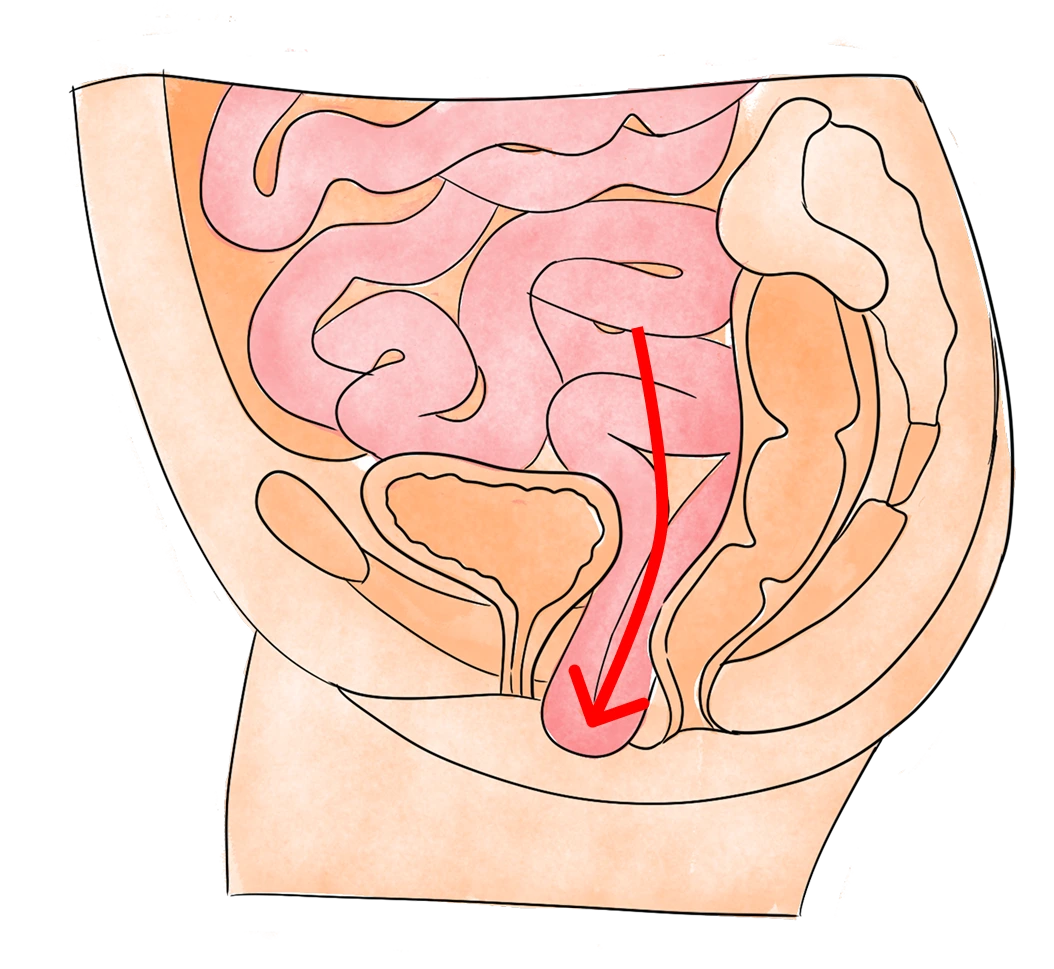
Bulging of the bladder into the front wall of the vagina.
A cystocele occurs when the bladder drops from its normal position and bulges into the front wall of the vagina. This can lead to pelvic pressure, urinary incontinence, frequent urgency, or difficulty fully emptying the bladder.
If you’re experiencing pelvic, bladder, or bowel pain, call us today to schedule a free appointment.
Early intervention leads to better outcomes.
Pelvic organ prolapse can interfere with bladder, bowel, and sexual function—and often impacts physical activity, intimacy, and self-confidence.
Without proper treatment, symptoms may worsen over time. Early, conservative intervention can delay or prevent the need for surgery, improve pelvic support, and significantly reduce symptoms.
Pelvic health physical therapy offers a safe, non-invasive, and effective approach to restoring muscle function, pressure regulation, and pelvic alignment.
At Pelvic Health Solutions, we offer private, full-hour sessions with licensed pelvic health physical therapists who specialize in treating sexual pain and pelvic dysfunction.
Your comfort, pace, and goals drive the care we provide.
Your personalized treatment may include:
We are Florida’s leading pelvic health physical therapy clinic, with locations in Palm Beach Gardens, Boca Raton, Stuart and Pembroke Pines. Our team is known for compassionate, trauma-informed care that integrates clinical expertise with individualized care for long lasting results.
We treat all genders and life stages, including bladder and bowel dysfunction, intimacy-related pain, pre and postpartum changes, menopause, post surgical recovery, trauma, or chronic pelvic pain.
This was the best investment in my health I could have made.
For about a year—maybe longer—I was dealing with issues like not being able to hold my bladder – I remember literally running down the hallways because I couldn’t hold my bladder. It was constant. That, along with the painful sex, really impacted my quality of life. I was young, and no one around me was talking about it. I had no idea what was going on.
I have seen remarkable improvement and can now enjoy simple things like taking a walk and laughing without embarrassment. It feels good to exercise again, too!
—G.D.
I was pretty skeptical that this would work, as I had never heard of this type of physical therapy before. I had six, once a week appointments scheduled…I began to feel better after two!
–E.W.
Many women suffer with pain, bowel or bladder problems and don’t realize that pelvic floor physical therapy can help. Gaining a sense of control over a frustrating and often times debilitating condition is life changing.
–T.S.
Many patients come to us after feeling rushed, overlooked, or given a one-size-fits-all plan elsewhere. Exceptional pelvic health care requires time, expertise, and individualized attention—conditions that traditional insurance models simply don’t allow.
Our out-of-network structure is intentional. It allows us to deliver the level of care you deserve.
Patients often find that investing in specialized, expert-led care leads to faster, more meaningful improvement—and ultimately reduces the time, cost, and frustration spent on ineffective or fragmented treatments.
At Pelvic Health Solutions, you receive care designed around you: private, precise, and rooted in clinical excellence.
Pelvic health physical therapy is a specialized area of physical therapy that focuses on assessing and treating conditions related to the pelvic floor muscles, ligaments, and connective tissues. The pelvic floor plays a crucial role in supporting the pelvic organs, controlling bladder and bowel function, and contributing to sexual health.
Pelvic health physical therapy focuses on the muscles, tissues, and organs specifically in the pelvic area, which include the bladder and bowel. It helps with problems like pelvic pain, urinary or bowel issues, and discomfort during sex.
Orthopedic physical therapy, on the other hand, deals with muscles and joints in other parts of the body, like the arms, legs, and back, to help with pain, stiffness, and injuries in those areas.
pulvinar dapibus leo.
elvic floor physical therapy applies to individuals with a range of symptoms. Some of the most common ones we see are:
Pelvic Pain: Chronic pelvic pain, pain during intercourse (dyspareunia), tailbone pain, or pain in the pelvic region with movement, sitting, or pressure.
Urinary Symptoms: Urinary incontinence (leakage of urine), urinary urgency or frequency, difficulty emptying the bladder, or nocturia (excessive nighttime urination).
Bowel Symptoms: Fecal incontinence (involuntary leakage of stool or gas), constipation, rectal pain/spasms, or difficulty with bowel movements.
Pregnancy and Postpartum: Pelvic health physical therapy can help prepare the pelvic floor for childbirth and address postpartum issues such as pelvic organ prolapse, perineal pain, or diastasis recti.
Pelvic Organ Prolapse: Descending or bulging of pelvic organs (such as the bladder, uterus, or rectum) into the vaginal canal.
Male Pelvic Conditions: Chronic pelvic pain in men, chronic prostatitis, and post-prostatectomy
If you’re considering scheduling your first visit, here’s what you can expect during the initial evaluation:
A comprehensive and respectful conversation
We begin by listening. All appointments are one-on-one with a dedicated pelvic floor physical therapist, in a private treatment room, for a full hour.
In your first session, your therapist will conduct a detailed medical and lifestyle history to better understand your symptoms, goals, and day-to-day function. Topics may include bladder, bowel, and sexual health—always discussed with care, professionalism, and respect for your comfort.
Clinical education tailored to you
You’ll receive clear, expert guidance on how the pelvic floor works, what may be contributing to your symptoms, and how physical therapy can help. Research shows that patients who understand their conditions have better outcomes. We prioritize education, and not just exercises, in your care so that you understand the why and how of your symptoms.
A thorough assessment
We assess posture, movement patterns, core stability, hip strength, breathing, and pelvic alignment. With your consent, we may offer an external and internal pelvic floor exam to assess strength, tone, and coordination. This is always optional and based on your comfort.
A personalized treatment plan
Before the session ends, your therapist will walk you through their findings and recommend a tailored and individualized plan for therapy — outlining what care may look like in the weeks ahead.
Our care model is centered around one-on-one treatment, clinical excellence, and compassionate support. We’re referred by over 100 doctors and have helped more than 5000 patients restore function, reduce symptoms, and feel confident in their bodies again.
Don’t struggle with your symptoms alone. Reach out to speak with one of our pelvic floor physical therapists.
Just like other therapies, it takes time and consistency to notice improvement. Healing time varies for each person. Some people might start feeling better after a few sessions, while others might need more time. It depends on how severe your symptoms are and how well you stick to your treatment plan.
Typically, we see our patients 1-2 times per week in order to make the most optimal recovery. Your therapist will work with you to create a plan that fits your needs and that helps you feel better as soon as possible!